COVID: Seven reasons mask wearing in the west was unnecessarily delayed

Masks help prevent the spread of SARS-CoV-2, the virus that causes COVID-19, yet masking policies in the west have featured some spectacular policy wrong turns, says Professor Trish Greenhalgh.
 ©
Photo by Nathan Dumlao on Unsplash
©
Photo by Nathan Dumlao on Unsplash
1. Ignoring Asia
Early studies showed that countries (mostly Asian) that made mask-wearing mandatory within 30 days of the first case emerging had dramatically fewer COVID-19 cases than those (mostly western) that delayed beyond 100 days. Rather than taking seriously the theory that the masking may have contributed to the low death rate, western countries dismissed mask-wearing as a cultural quirk of so-called collectivist societies or as a folk myth among the less educated.
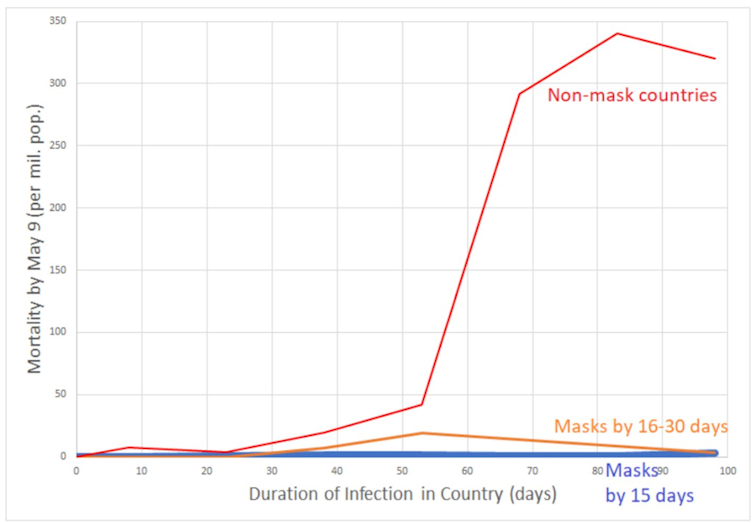 The impact of delaying mask mandates. Trish Greenhalgh, Author provided
The impact of delaying mask mandates. Trish Greenhalgh, Author provided2. Waiting for perfect evidence
Whereas Asian countries introduced masks early just in case they were effective (the precautionary principle), those in the west argued that the best course of action in the face of uncertain evidence was to do nothing. Such caution is appropriate for trials of new drugs and vaccines, which may have side-effects worse than the disease itself. But a bit of cloth over the face simply doesn’t have the same risks, and delay could conceivably cause huge harm.
Instead of asking: “Do we have definitive evidence that masks work?”, we should have asked: “What should we do in a rapidly escalating pandemic, given the empirical uncertainty?”
3. Inflating speculative harms
Some feared that masks might act as “fomites” (objects that carry disease) because people would constantly fiddle with the mask (which may have infected droplets on the outside) and then touch their eyes, thereby self-infecting. However, evidence shows that people actually touch their face less when wearing masks than when unmasked. But masking was depicted as a highly specialist and potentially dangerous activity that depended on perfect donning and doffing procedures.
The concern about “risk-compensation” (if you wear a mask, you’ll feel protected and take more risks, like a driver who becomes more reckless when wearing a seatbelt) was also unsupported by evidence.
4. Over-valuing randomised controlled trial evidence
In the name of evidence-based medicine, the west became obsessed with the holy grail of a definitive randomised controlled trial (RCT) that would quantify both the benefits and the harms of masks, just as you would for a drug. But RCTs of masks – in which people are randomly allocated to wearing or not wearing a mask and then followed up to see who gets infected – are problematic.
First, they can’t measure source control (how much my mask-wearing protects you from becoming infected). I consent to wearing a mask, and I also consent to you testing me to see if I become infected. But to test whether I’ve passed the virus on to others, the whole town must consent to be tested (at the start of the trial and repeatedly) for infection – and this is not feasible.
Second, RCTs undertaken over short timescales can’t capture exponential changes in transmission. A mere 10% reduction in viral transmission rate can, over repeated reproduction cycles, lead to a halving of total cases. But a short-term RCT will measure only that initial 10% reduction and deem it “statistically non-significant”.
While RCTs have been a godsend for drugs and vaccines, they’ve distracted and misled us on masks.
5. Under-valuing mechanistic evidence
When assessing a complex phenomenon unfolding in a complex system, we need two kinds of evidence: mechanistic evidence to help us understand the causal pathways that link an intervention (such as mask-wearing) to a particular outcome (such as not catching COVID-19) and statistical evidence to estimate the size of the effect.
Mechanistic evidence is often generated in laboratories. For example, measuring the droplet clouds induced by sneezing or using an artificial cough simulator to test the filtration efficacy of different kinds of masks. These studies do not prove that masks work, but they are important pieces of a wider jigsaw and should not have been dismissed.
6. Denying airborne spread
There is an extensive body of evidence that airborne spread is the main mode of transmission of SARS-CoV-2, through super-spreader events in under-ventilated indoor spaces. This is a game-changer. It means we need to avoid close contact (airborne spread occurs mostly within two metres), prolonged time indoors and crowds.
With masks, we need to shift our mechanistic model from one that focuses on projectile clouds of droplets (coughs and sneezes) to one that sees the very air we breathe as laden with infectious particles. For a long time, the World Health Organization denied the airborne nature of this virus. Yet airborne spread matters for mask design because it means we need to pay meticulous attention to mask fit (to avoid any gaps around the side where air can escape) and perhaps consider upgrading to a higher-grade FFP2 mask.
7. Prematurely withdrawing mask mandates
The UK government’s announcement that masks will cease to be compulsory in public places from July 19 is premature. Cases of COVID-19 are rising rapidly and while vaccination has weakened the link with hospitalisation and death, these numbers are also on the rise. If politicians are keen to “open up” society despite these continuing risks, continuing compulsory masking could be one way to do so more safely.
This article is republished from The Conversation under a Creative Commons license. Read the original article.